- Pathophysiology of hypertension
-
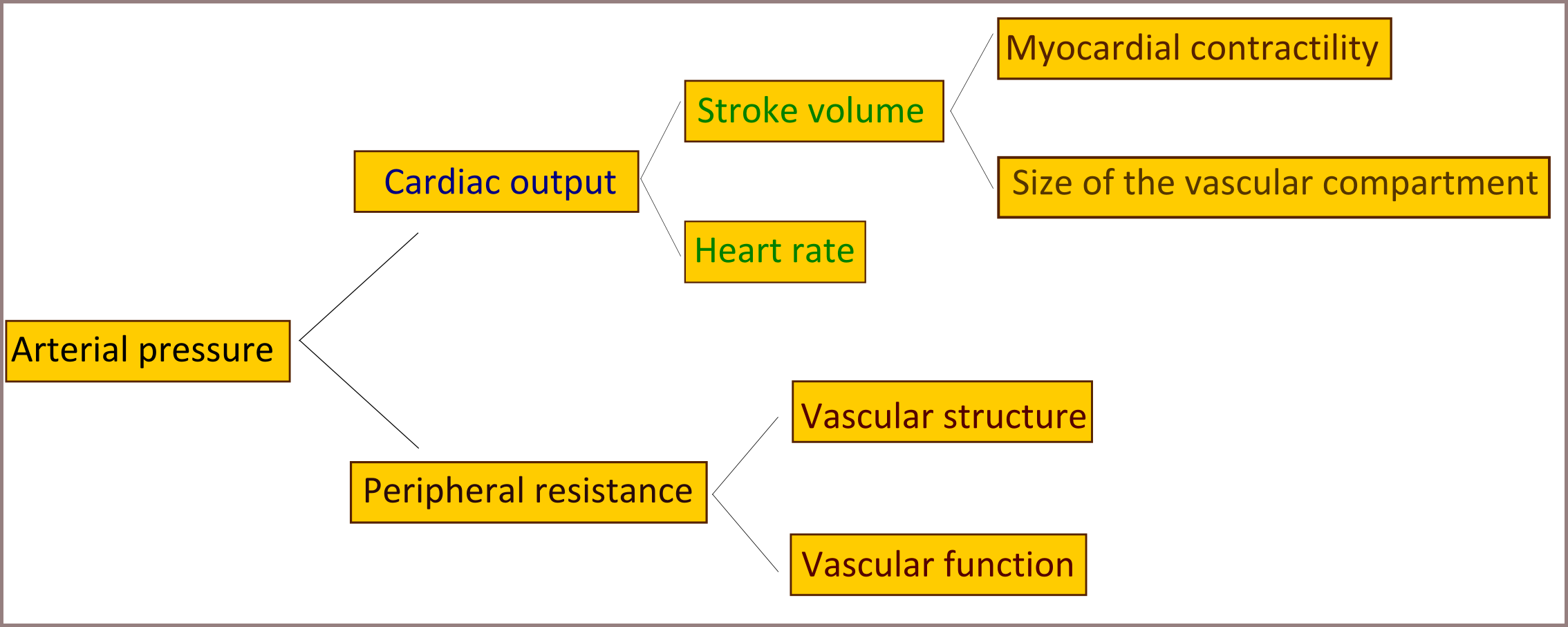
 A diagram explaining factors affecting arterial pressure
A diagram explaining factors affecting arterial pressure
The pathophysiology of hypertension is an area of active research, attempting to explain causes of hypertension, which is a chronic disease characterized by elevation of blood pressure. Hypertension can be classified as either essential or secondary. Essential hypertension indicates that no specific medical cause can be found to explain a patient's condition. About 90-95% of hypertension is essential hypertension.[1][2][3][4] Secondary hypertension indicates that the high blood pressure is a result of another underlying condition, such as kidney disease or tumours (adrenal adenoma or pheochromocytoma). Persistent hypertension is one of the risk factors for strokes, heart attacks, heart failure and arterial aneurysm, and is a leading cause of chronic renal failure.[5]
Most mechanisms leading to secondary hypertension are well understood. The pathophysiology of essential hypertension remains an area of active research, with many theories and different links to many risk factors.
Cardiac output and peripheral resistance are the two determinants of arterial pressure.[6] Cardiac output is determined by stroke volume and heart rate; stroke volume is related to myocardial contractility and to the size of the vascular compartment. Peripheral resistance is determined by functional and anatomic changes in small arteries and arterioles.
Contents
Genetics
Evidence for genetic influence on blood pressure comes from various sources.[7] There is greater similarity in blood pressure within families than between families, which indicates a form of inheritance.[8] And it was proved that this finding wasn't due to shared environmental factors.[9] Single gene mutations is proved to cause Mendelian forms of high and low blood pressure.[10] almost 10 genes have been identified to cause this forms of hypertension.[10][11] These mutations affect blood pressure by altering renal salt handling.[12] Recently and with the aid of newly developed genetic analysis techniques researchers found statistically significant linkage of blood pressure to several chromosomal regions, including regions linked to familial combined hyperlipidemia.[13][14][15][16][17] These findings suggest that there are many genetic loci, each with small effects on blood pressure in the general population. Overall, however, identifiable single-gene causes of hypertension are uncommon, consistent with a multifactorial cause of essential hypertension.[2][7][18][19]
The best studied monogenic cause of hypertension is the Liddle syndrome, a rare but clinically important disorder in which constitutive activation of the epithelial sodium channel predisposes to severe, treatment-resistant hypertension.[20] Epithelial sodium channel activation resulting in inappropriate sodium retention at the renal collecting duct level. Patients with the Liddle syndrome typically present with volume-dependent, low renin, and low aldosterone, and hypertension. Screenings of general hypertensive populations indicate that the Liddle syndrome is rare and does not contribute substantially to the development of hypertension in the general population.[21]
Autonomic nervous system
Also the autonomic nervous system, plays a central role in maintaining the cardiovascular homeostasis via pressure, volume, and chemoreceptor signals. Done by altering peripheral vasculature, and kidneys, causing increased cardiac output, increased vascular resistance, and fluid retention. Disorder of the system, as in case of sympathetic nervous system overactivity, increases blood pressure and contributes to the development and maintenance of hypertension.[22][23][24][25] In addition, autonomic imbalance (i.e. increased sympathetic tone accompanied by reduced parasympathetic tone) has been associated with many metabolic and hemodynamic abnormalities that result in increased cardiovascular morbidity and mortality.[24][26]
The mechanisms of increased sympathetic nervous system activity in hypertension are complex and involve alterations in baroreflex and chemoreflex pathways at both peripheral and central levels. Arterial baroreceptors are reset to a higher pressure in hypertensive patients, and this peripheral resetting reverts to normal when arterial pressure is normalized.[8][27][28] Furthermore, there is central resetting of the aortic baroreflex in hypertensive patients, resulting in suppression of sympathetic inhibition after activation of aortic baroreceptor nerves. This baroreflex resetting seems to be mediated, at least partly, by a central action of angiotensin II.[29][30][31] Additional small-molecule mediators that suppress baroreceptor activity and contribute to exaggerated sympathetic drive in hypertension include reactive oxygen species and endothelin.[32][33] Some studies shown that hypertensive patients manifest greater vasoconstrictor responses to infused norepinephrine than normotensive controls.[34] And that hypertensive patients doesn't show the normal response to increased circulating norepinephrine levels which generally induces downregulation of noradrenergic receptor, and its believed that this abnormal response is genetically inherited.[35]
Exposure to stress increases sympathetic outflow, and repeated stress-induced vasoconstriction may result in vascular hypertrophy, leading to progressive increases in peripheral resistance and blood pressure.[2] This could partly explain the greater incidence of hypertension in lower socioeconomic groups, since they must endure greater levels of stress associated with daily living. Persons with a family history of hypertension manifest augmented vasoconstrictor and sympathetic responses to laboratory stressors, such as cold pressor testing and mental stress, that may predispose them to hypertension. This is particularly true of young African Americans. Exaggerated stress responses may contribute to the increased incidence of hypertension in this group.[36]
Renin-angiotensin-aldosterone system
Another system maintaining the extracellular fluid volume, peripheral resistance and that if disturbed may lead to hypertension, is the renin-angiotensin-aldosterone system. Renin is a circulating enzyme that participates in maintaining extracellular volume, and arterial vasoconstriction, Thus it contributing to regulation of the blood pressure, it performs this function through breaking down (hydrolyzes) angiotensinogen secreted from the liver into the peptide angiotensin I, Angiotensin I is further cleaved by an enzyme that is located primarily but not exclusively in the pulmonary circulation bound to endothelium, that enzyme is angiotensin converting enzyme (ACE) producing angiotensin II, the most vasoactive peptide.[37][38] Angiotensin II is a potent constrictor of all blood vessels. It acts on the musculature of arteries and thereby raises the peripheral resistance, and so elevates blood pressure. Angiotensin II also acts on the adrenal glands too and releases Aldosterone, which stimulates the epithelial cells of the kidneys to increase re-absorption of salt and water leading to raised blood volume and raised blood pressure. So elevation of renin level in the blood, which is normally in adult human is 1.98-24.6 ng/L in the upright position.[39] will lead to hypertension.[2][40]
Recent studies claims that obesity is a risk factor for hypertension because of activation of the renin-angiotensin system (RAS) in adipose tissue,[41][42] and also linked renin-angiotensin system with insulin resistance, and claims that anyone can cause the other.[43] Local production of angiotensin II in various tissues, including the blood vessels, heart, adrenals, and brain, is controlled by ACE and other enzymes, including the serine proteinase chymase. The activity of local renin–angiotensin systems and alternative pathways of angiotensin II formation may make an important contribution to remodeling of resistance vessels and the development of target organ damage (i.e. left ventricular hypertrophy, congestive heart failure, atherosclerosis, stroke, end-stage renal disease, myocardial infarction, and arterial aneurysm) in hypertensive persons.[40]
Endothelial dysfunction
The endothelium of blood vessels produces an extensive range of substances that influence blood flow and, in turn, is affected by changes in the blood and the pressure of blood flow. For example, local nitric oxide and endothelin, which are secreted by the endothelium, are the major regulators of vascular tone and blood pressure. In patients with essential hypertension, the balance between the vasodilators and the vasoconstrictors is upset, which leads to changes in the endothelium and sets up a “vicious cycle” that contributes to the maintenance of high blood pressure. In patients with hypertension, endothelial activation and damage also lead to changes in vascular tone, vascular reactivity, and coagulation and fibrinolytic pathways. Alterations in endothelial function are a reliable indicator of target organ damage and atherosclerotic disease, as well as prognosis.[44]
Multiple evidences suggest that oxidant stress alters many functions of the endothelium, including modulation of vasomotor tone. Inactivation of nitric oxide (NO) by superoxide and other reactive oxygen species (ROS) seems to occur in conditions such as hypertension.[45][46][47] Normally nitric oxide is an important regulator and mediator of numerous processes in the nervous, immune and cardiovascular systems, including smooth muscle relaxation thus resulting in vasodilation of the artery and increasing blood flow, suppressor of migration and proliferation of vascular smooth-muscle cells.[2] It has been suggested that angiotensin II enhances formation of the oxidant superoxide at concentrations that affect blood pressure minimally.[48]
Endothelin is a potent vasoactive peptide produced by endothelial cells that has both vasoconstrictor and vasodilator properties. Circulating endothelin levels are increased in some hypertensive patients,[49][49][50] particularly African Americans and persons with hypertension.[49][51][52][53]
References
- ^ Carretero OA, Oparil S (January 2000). "Essential hypertension. Part I: definition and etiology". Circulation 101 (3): 329–35. doi:10.1161/01.CIR.101.3.329. PMID 10645931. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=10645931. Retrieved 2009-06-05.
- ^ a b c d e Oparil S, Zaman MA, Calhoun DA (November 2003). "Pathogenesis of hypertension". Ann. Intern. Med. 139 (9): 761–76. PMID 14597461.
- ^ Hall, John E.; Guyton, Arthur C. (2006). Textbook of medical physiology. St. Louis, Mo: Elsevier Saunders. pp. 228. ISBN 0-7216-0240-1.
- ^ "Hypertension: eMedicine Nephrology". http://emedicine.medscape.com/article/241381-overview. Retrieved 2009-06-05.
- ^ Pierdomenico SD, Di Nicola M, Esposito AL, et al. (June 2009). "Prognostic Value of Different Indices of Blood Pressure Variability in Hypertensive Patients". American Journal of Hypertension 22 (8): 842–7. doi:10.1038/ajh.2009.103. PMID 19498342.
- ^ Klabunde, Richard E. (2007). "Cardiovascular Physiology Concepts - Mean Arterial Pressure". http://www.cvphysiology.com/Blood%20Pressure/BP006.htm. Retrieved 2008-09-29.
- ^ a b Corvol P, Persu A, Gimenez-Roqueplo AP, Jeunemaitre X (June 1999). "Seven lessons from two candidate genes in human essential hypertension: angiotensinogen and epithelial sodium channel". Hypertension 33 (6): 1324–31. PMID 10373210. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=10373210. Retrieved 2009-06-08.
- ^ a b Feinleib M, Garrison RJ, Fabsitz R, et al. (October 1977). "The NHLBI twin study of cardiovascular disease risk factors: methodology and summary of results". American Journal of Epidemiology 106 (4): 284–5. PMID 562066. http://aje.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=562066. Retrieved 2009-06-08.
- ^ Biron P, Mongeau JG, Bertrand D (October 1976). "Familial aggregation of blood pressure in 558 adopted children". Canadian Medical Association Journal 115 (8): 773–4. PMC 1878814. PMID 974967. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1878814.
- ^ a b Lifton RP, Gharavi AG, Geller DS (February 2001). "Molecular mechanisms of human hypertension". Cell 104 (4): 545–56. doi:10.1016/S0092-8674(01)00241-0. PMID 11239411. http://linkinghub.elsevier.com/retrieve/pii/S0092-8674(01)00241-0. Retrieved 2009-06-08.
- ^ Wilson FH, Disse-Nicodème S, Choate KA, et al. (August 2001). "Human hypertension caused by mutations in WNK kinases". Science 293 (5532): 1107–12. doi:10.1126/science.1062844. PMID 11498583. http://www.sciencemag.org/cgi/pmidlookup?view=long&pmid=11498583. Retrieved 2009-06-08.
- ^ Guyton AC (June 1991). "Blood pressure control--special role of the kidneys and body fluids". Science 252 (5014): 1813–6. doi:10.1126/science.2063193. PMID 2063193. http://www.sciencemag.org/cgi/pmidlookup?view=long&pmid=2063193. Retrieved 2009-06-08.
- ^ Hsueh WC, Mitchell BD, Schneider JL, et al. (June 2000). "QTL influencing blood pressure maps to the region of PPH1 on chromosome 2q31-34 in Old Order Amish". Circulation 101 (24): 2810–6. PMID 10859286. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=10859286. Retrieved 2009-06-08.
- ^ Levy D, DeStefano AL, Larson MG, et al. (October 2000). "Evidence for a gene influencing blood pressure on chromosome 17. Genome scan linkage results for longitudinal blood pressure phenotypes in subjects from the framingham heart study". Hypertension 36 (4): 477–83. PMID 11040222. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=11040222. Retrieved 2009-06-08.
- ^ Kristjansson K, Manolescu A, Kristinsson A, et al. (June 2002). "Linkage of essential hypertension to chromosome 18q". Hypertension 39 (6): 1044–9. doi:10.1161/01.HYP.0000018580.24644.18. PMID 12052839. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=12052839. Retrieved 2009-06-08.
- ^ Hunt SC, Ellison RC, Atwood LD, Pankow JS, Province MA, Leppert MF (July 2002). "Genome scans for blood pressure and hypertension: the National Heart, Lung, and Blood Institute Family Heart Study". Hypertension 40 (1): 1–6. doi:10.1161/01.HYP.0000022660.28915.B1. PMID 12105129. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=12105129. Retrieved 2009-06-08.
- ^ Selby JV, Newman B, Quiroga J, Christian JC, Austin MA, Fabsitz RR (April 1991). "Concordance for dyslipidemic hypertension in male twins". JAMA : the Journal of the American Medical Association 265 (16): 2079–84. doi:10.1001/jama.265.16.2079. PMID 2013927.
- ^ Niu T, Yang J, Wang B, et al. (February 1999). "Angiotensinogen gene polymorphisms M235T/T174M: no excess transmission to hypertensive Chinese". Hypertension 33 (2): 698–702. PMID 10024331. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=10024331. Retrieved 2009-06-08.
- ^ Luft FC (May 2000). "Molecular genetics of human hypertension". Current Opinion in Nephrology and Hypertension 9 (3): 259–66. doi:10.1097/00041552-200005000-00009. PMID 10847327. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=1062-4821&volume=9&issue=3&spage=259. Retrieved 2009-06-08.
- ^ Shimkets RA, Warnock DG, Bositis CM, et al. (November 1994). "Liddle's syndrome: heritable human hypertension caused by mutations in the beta subunit of the epithelial sodium channel". Cell 79 (3): 407–14. doi:10.1016/0092-8674(94)90250-X. PMID 7954808. http://linkinghub.elsevier.com/retrieve/pii/0092-8674(94)90250-X. Retrieved 2009-06-08.
- ^ Melander O, Orho M, Fagerudd J, et al. (May 1998). "Mutations and variants of the epithelial sodium channel gene in Liddle's syndrome and primary hypertension". Hypertension 31 (5): 1118–24. PMID 9576123. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=9576123. Retrieved 2009-06-08.
- ^ Somers VK, Anderson EA, Mark AL (January 1993). "Sympathetic neural mechanisms in human hypertension". Current Opinion in Nephrology and Hypertension 2 (1): 96–105. doi:10.1097/00041552-199301000-00015. PMID 7922174.
- ^ Takahashi H (August 2008). "[Sympathetic hyperactivity in hypertension]" (in Japanese). Nippon Rinsho. Japanese Journal of Clinical Medicine 66 (8): 1495–502. PMID 18700548.
- ^ a b Esler M (June 2000). "The sympathetic system and hypertension". American Journal of Hypertension 13 (6 Pt 2): 99S–105S. doi:10.1016/S0895-7061(00)00225-9. PMID 10921528.
- ^ Mark AL (December 1996). "The sympathetic nervous system in hypertension: a potential long-term regulator of arterial pressure". Journal of Hypertension. Supplement : Official Journal of the International Society of Hypertension 14 (5): S159–65. PMID 9120673.
- ^ Brook RD, Julius S (June 2000). "Autonomic imbalance, hypertension, and cardiovascular risk". American Journal of Hypertension 13 (6 Pt 2): 112S–122S. doi:10.1016/S0895-7061(00)00228-4. PMID 10921530.
- ^ Guo GB, Thames MD, Abboud FM (August 1983). "Arterial baroreflexes in renal hypertensive rabbits. Selectivity and redundancy of baroreceptor influence on heart rate, vascular resistance, and lumbar sympathetic nerve activity". Circulation Research 53 (2): 223–34. PMID 6883646. http://circres.ahajournals.org/cgi/pmidlookup?view=long&pmid=6883646. Retrieved 2009-06-08.
- ^ Xie PL, Chapleau MW, McDowell TS, Hajduczok G, Abboud FM (August 1990). "Mechanism of decreased baroreceptor activity in chronic hypertensive rabbits. Role of endogenous prostanoids". The Journal of Clinical Investigation 86 (2): 625–30. doi:10.1172/JCI114754. PMC 296770. PMID 2117025. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=296770.
- ^ Lohmeier TE (June 2001). "The sympathetic nervous system and long-term blood pressure regulation". American Journal of Hypertension 14 (6 Pt 2): 147S–154S. doi:10.1016/S0895-7061(01)02082-9. PMID 11411750.
- ^ Guo GB, Abboud FM (May 1984). "Impaired central mediation of the arterial baroreflex in chronic renal hypertension". The American Journal of Physiology 246 (5 Pt 2): H720–7. PMID 6720985. http://ajpheart.physiology.org/cgi/pmidlookup?view=long&pmid=6720985. Retrieved 2009-06-08.
- ^ Abboud FM (February 1974). "Effects of sodium, angiotensin, and steroids on vascular reactivity in man". Federation Proceedings 33 (2): 143–9. PMID 4359754.
- ^ Li Z, Mao HZ, Abboud FM, Chapleau MW (October 1996). "Oxygen-derived free radicals contribute to baroreceptor dysfunction in atherosclerotic rabbits". Circulation Research 79 (4): 802–11. PMID 8831504. http://circres.ahajournals.org/cgi/pmidlookup?view=long&pmid=8831504. Retrieved 2009-06-08.
- ^ Chapleau MW, Hajduczok G, Abboud FM (July 1992). "Suppression of baroreceptor discharge by endothelin at high carotid sinus pressure". The American Journal of Physiology 263 (1 Pt 2): R103–8. PMID 1636777. http://ajpregu.physiology.org/cgi/pmidlookup?view=reprint&pmid=1636777. Retrieved 2009-06-08.
- ^ Ziegler MG, Mills P, Dimsdale JE (July 1991). "Hypertensives' pressor response to norepinephrine. Analysis by infusion rate and plasma levels". American Journal of Hypertension 4 (7 Pt 1): 586–91. PMID 1873013.
- ^ Bianchetti MG, Beretta-Piccoli C, Weidmann P, Ferrier C (April 1986). "Blood pressure control in normotensive members of hypertensive families". Kidney International 29 (4): 882–8. doi:10.1038/ki.1986.81. PMID 3520094.
- ^ Calhoun DA, Mutinga ML, Collins AS, Wyss JM, Oparil S (December 1993). "Normotensive blacks have heightened sympathetic response to cold pressor test". Hypertension 22 (6): 801–5. PMID 8244512. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=8244512. Retrieved 2009-06-09.
- ^ Fujino T, Nakagawa N, Yuhki K, et al. (September 2004). "Decreased susceptibility to renovascular hypertension in mice lacking the prostaglandin I2 receptor IP". J. Clin. Invest. 114 (6): 805–12. doi:10.1172/JCI21382. PMC 516260. PMID 15372104. http://www.jci.org/cgi/content/full/114/6/805?ijkey=e3335f0a9a7b40386d49e7172910ea6345c9342a.
- ^ Brenner & Rector's The Kidney, 7th ed., Saunders, 2004. pp.2118-2119.Full Text with MDConsult subscription
- ^ Hamilton Regional Laboratory Medicine Program - Laboratory Reference Centre Manual. Renin Direct
- ^ a b McConnaughey MM, McConnaughey JS, Ingenito AJ (June 1999). "Practical considerations of the pharmacology of angiotensin receptor blockers". Journal of Clinical Pharmacology 39 (6): 547–59. doi:10.1177/00912709922008155. PMID 10354958. http://jcp.sagepub.com/cgi/pmidlookup?view=long&pmid=10354958. Retrieved 2009-06-09.
- ^ Segura J, Ruilope LM (October 2007). "Obesity, essential hypertension and renin-angiotensin system". Public Health Nutrition 10 (10A): 1151–5. doi:10.1017/S136898000700064X. PMID 17903324. http://journals.cambridge.org/abstract_S136898000700064X. Retrieved 2009-06-02.
- ^ Hasegawa H, Komuro I (April 2009). "[The progress of the study of RAAS]" (in Japanese). Nippon Rinsho. Japanese Journal of Clinical Medicine 67 (4): 655–61. PMID 19348224.
- ^ Saitoh S (April 2009). "[Insulin resistance and renin-angiotensin-aldosterone system]" (in Japanese). Nippon Rinsho. Japanese Journal of Clinical Medicine 67 (4): 729–34. PMID 19348235.
- ^ O'Brien, Eoin; Beevers, D. G.; Lip, Gregory Y. H. (2007). ABC of hypertension. London: BMJ Books. ISBN 1-4051-3061-X.
- ^ Nakazono K, Watanabe N, Matsuno K, Sasaki J, Sato T, Inoue M (November 1991). "Does superoxide underlie the pathogenesis of hypertension?". Proceedings of the National Academy of Sciences of the United States of America 88 (22): 10045–8. doi:10.1073/pnas.88.22.10045. PMC 52864. PMID 1658794. http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=52864.
- ^ Laursen JB, Rajagopalan S, Galis Z, Tarpey M, Freeman BA, Harrison DG (February 1997). "Role of superoxide in angiotensin II-induced but not catecholamine-induced hypertension". Circulation 95 (3): 588–93. PMID 9024144. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=9024144. Retrieved 2009-06-09.
- ^ Cai H, Harrison DG (November 2000). "Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress". Circulation Research 87 (10): 840–4. PMID 11073878. http://circres.ahajournals.org/cgi/pmidlookup?view=long&pmid=11073878. Retrieved 2009-06-09.
- ^ Fukui T, Ishizaka N, Rajagopalan S, et al. (January 1997). "p22phox mRNA expression and NADPH oxidase activity are increased in aortas from hypertensive rats". Circulation Research 80 (1): 45–51. PMID 8978321. http://circres.ahajournals.org/cgi/pmidlookup?view=long&pmid=8978321. Retrieved 2009-06-09.
- ^ a b c Touyz RM, Schiffrin EL (June 2003). "Role of endothelin in human hypertension". Canadian Journal of Physiology and Pharmacology 81 (6): 533–41. doi:10.1139/y03-009. PMID 12839265. http://article.pubs.nrc-cnrc.gc.ca/ppv/RPViewDoc?issn=0008-4212&volume=81&issue=6&startPage=533. Retrieved 2009-06-09.
- ^ Shreenivas S, Oparil S (2007). "The role of endothelin-1 in human hypertension". Clinical Hemorheology and Microcirculation 37 (1–2): 157–78. PMID 17641406. http://iospress.metapress.com/openurl.asp?genre=article&issn=1386-0291&volume=37&issue=1&spage=157. Retrieved 2009-06-09.
- ^ Ergul S, Parish DC, Puett D, Ergul A (October 1996). "Racial differences in plasma endothelin-1 concentrations in individuals with essential hypertension". Hypertension 28 (4): 652–5. PMID 8843893. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=8843893. Retrieved 2009-06-09.
- ^ Grubbs AL, Ergul A (2001). "A review of endothelin and hypertension in African-American individuals". Ethnicity & Disease 11 (4): 741–8. PMID 11763297.
- ^ Campia U, Cardillo C, Panza JA (June 2004). "Ethnic differences in the vasoconstrictor activity of endogenous endothelin-1 in hypertensive patients". Circulation 109 (25): 3191–5. doi:10.1161/01.CIR.0000130590.24107.D3. PMID 15148269. http://circ.ahajournals.org/cgi/pmidlookup?view=long&pmid=15148269. Retrieved 2009-06-09.
Categories:- Hypertension
- Pathophysiology
- Cardiology
- Cardiovascular diseases
- Medical conditions related to obesity
Wikimedia Foundation. 2010.